Menopause Series Part 1: What You Missed Learning About Menopause
-180x180.png)
Authors: Shayda Swann, MD/PhD Candidate, University of British Columbia, Department of Medicine, Shannon Mahony, BSc, Human Biology, University of Toronto, Krembil Research Institute | Editors: Romina Garcia de leon (Blog Coordinator)
Published: October 6, 2023
*Throughout this series, we want to acknowledge that not all women will experience menopause, and not all folks who experience menopause identify as women. We understand that different terminology will suit different folks. We hope this information is helpful to folks of diverse genders and identities*
What comes to mind when you hear “menopause”? Hot flashes? Night sweats? Irritability? Are these symptoms normal? And what age should you expect to experience them? Do you just have to live with this discomfort? In this 3-part deep dive into menopause, we hope to dive into the information we’ve learned from our fellow experts to ensure this is a time in your life where you can navigate (and maybe even celebrate) this unique phase of life!
But first, let’s talk about what menopause actually is.Spontaneous menopause (often referred to as “natural” menopause) occurs when the ovaries gradually release lower levels of the reproductive hormones estradiol and progesterone. However, this process is not linear and hormone levels can fluctuate dramatically during this time (Figure 1). This transition phase is called perimenopause and typically occurs between ages 40-50. Because of the rapid and dynamic fluctuations in hormone levels, symptoms may be most severe during this time. Perimenopause typically lasts for 2-10 years and during this time women may have irregular periods, with shorter or longer cycles than usual.

Figure 1. Stages of Menopause Image credit: hertilityhealth.com
When periods have stopped for at least one year (not due to pregnancy/breastfeeding, hormonal contraceptive / other medication use, or other underlying medical conditions), a woman is considered to be in spontaneous menopause. The average age of menopause in Canada is 51 and typically occurs between ages 45-55. If your periods stop before age 45, it’s worthwhile speaking with your doctor to determine if you are experiencing early menopause or if you have another underlying health condition. In early menopause, individuals reach menopause before age 45 and progress through similar stages and hormone fluctuations as individuals in natural menopause. Premature menopause typically happens even earlier (before age 40) and diverges significantly from the typical menopause stages in that hormones fluctuate more erratically and some women may have return of menses. This type of menopause is the result of Primary Ovarian Insufficiency (POI), a condition where the ovaries stop working normally. It is believed that both premature and early menopause may be due to a variety of genetic and lifestyle factors.
It’s also important to mention that menopause can be induced by the removal of both ovaries, known as a bilateral oophorectomy, which is also referred to as surgical menopause. This results in abrupt changes in circulating hormone levels within 24 hours. These surgeries can be to treat ovarian conditions such as endometriosis and/or for the treatment and/or prevention of cancer. Women that experience this type of menopause tend to report more severe and abrupt menopause symptoms compared to women that are spontaneously menopausal.
Lastly, we have spontaneous postmenopause (sometimes also called menopause). This is the time between the final menstrual period and the rest of a woman’s life. This is when estradiol and progesterone will be at their lowest. At this phase, some menopausal symptoms that are caused by hormone fluctuations, like hot flashes and night sweats, tend to subside. Other symptoms that are caused by low hormone levels, like vaginal dryness, might continue to worsen. The risk of cardiovascular disease, osteoporosis, and the genitourinary syndrome of menopause also tend to increase at this stage due to the loss of those protective hormones.
Importantly, menopause will typically last for one-third to one-half of a woman’s life. So why don’t we know more about it? The Menopause Foundation of Canada decided to investigate this knowledge gap by surveying more than 1,000 Canadian women aged 40-60 from representative regions, educations, incomes, and ethnicities. Their results are summarized in the landmark 2022 report, The Silence and the Stigma: Menopause in Canada. Despite more than one quarter of Canadian women being perimenopausal or menopausal, they found that “menopause is overwhelmingly viewed as negative and remains shrouded in secrecy.” So let’s shed some light on this experience!
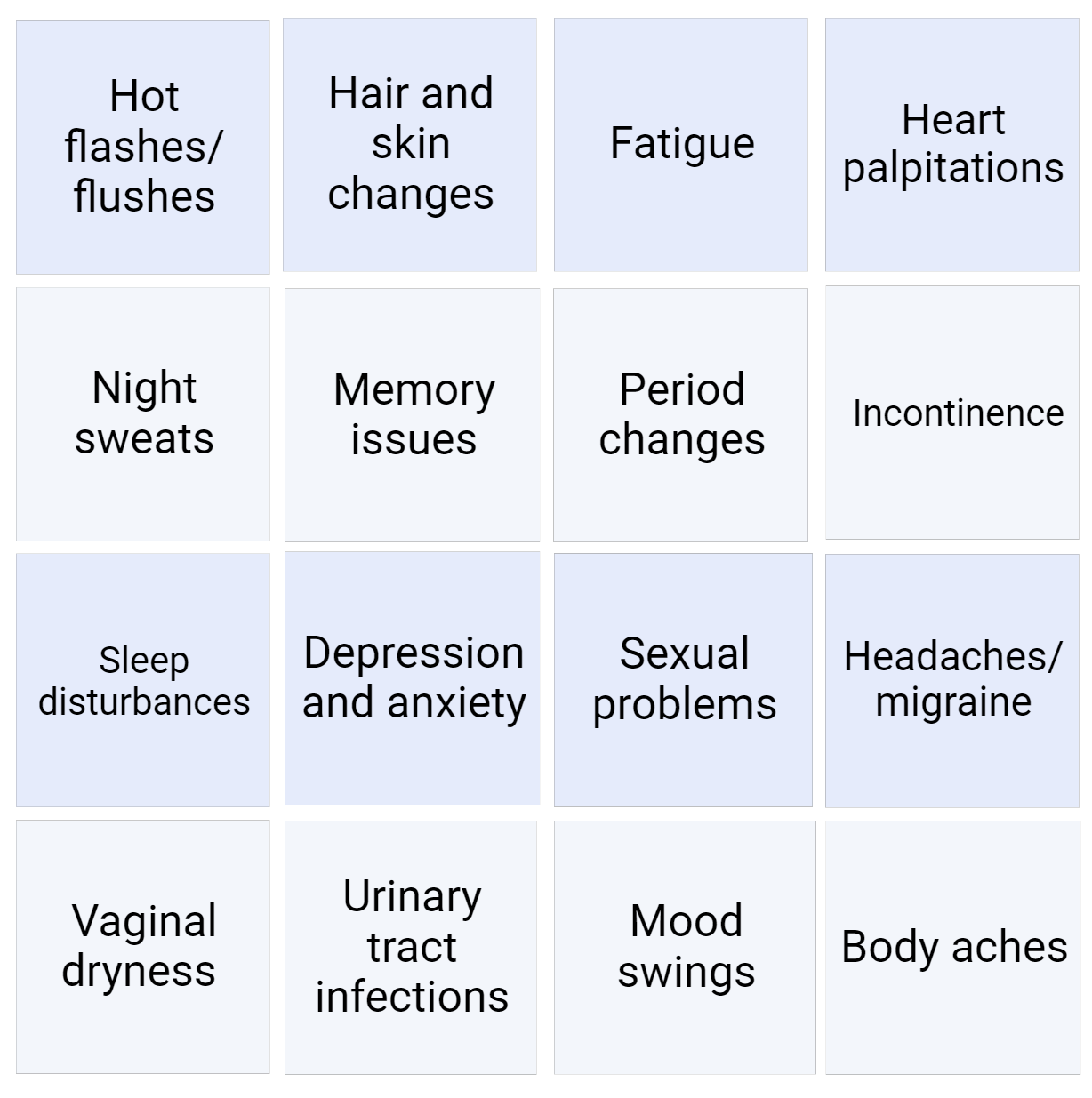
First, the report dives into menopause symptoms that can occur with all types of menopause. You might be surprised to learn that there are more than 30 symptoms of menopause (Figure 2), and while 84% of women were aware of hot flashes and 77% about night sweats, the majority did not know that urinary tract infections, heart palpitations, body aches, headaches/migraine, anxiety, depression, memory issues, and pain during sexual intercourse were all potential symptoms of menopause. In the report, women reported experiencing an average of seven symptoms. Unfortunately, one-third of women felt that their symptoms were undertreated, despite the availability of effective treatments.
Figure 2. Common Symptoms of Menopause Created using BioRender. Check out the
The Silence and the Stigma report also highlights the challenges women face within the medical system, in their intimate relationships, and in the workplace during menopause. More than half of respondents felt that menopause is “taboo”, and a similar proportion felt unprepared for their menopause journey, leading to feelings of isolation and loneliness. Unfortunately, only 40% of women sought treatment for their symptoms and 72% of those who did found that the medical advice was not helpful or only somewhat helpful. These experiences also impact women’s quality of life and relationships, with 41% of women reporting that menopause negatively impacted their relationship with their significant other. It also affects women’s experiences in the workplace, with three-quarters reporting that their employer was not supportive or did not know if they offered support in helping them to cope with symptoms.
As Dr. Wendy Wolfman, MD, FRCS(C), FACOG, NCMP noted in the report, “Menopause is seen as something women must endure, like a woman’s burden. This is unacceptable.” In the next part of this series, we will go through the history of menopause hormone therapy and current research in this field. Our third blog will go more into detail about options for menopause treatments, including hormonal, non-hormonal, and lifestyle options. Stay tuned for these blogs and connect with us on social media to share your experiences of menopause, questions about treatment, or share feedback on this series!
-180x180.png)

